Electronic data interchange, or EDI, is a standardized, digital exchange of structured healthcare data between providers, clearinghouses, and payers. The data exchange for EDIs requires a secure computer-to-computer network and plays an essential role in digital medical billing.
EDI transactions are used for eligibility checks, claim submissions, claim status inquiries, and remittance advice sent from payers to providers. According to the Department of Health & Human Services (HHS)’s guidance on adopted standards, HIPAA mandates the use of standardized formats for covered transactions when they are conducted electronically, establishing national standards for interoperability and healthcare administrative transactions. But what are these standards, and how do EDIs work?
In this article, we’ll discuss EDI in healthcare, the transaction process, state-level nuances that negatively impact billers, and expected rule changes in 2028 and beyond.
Note: Clearinghouses act as intermediaries that validate, format, and route EDI transactions between providers and payers.
What is EDI Reporting?
EDI reporting refers to the acknowledgments and response files generated after an EDI transaction is submitted. According to the CMS, these acknowledgements include the following:
- TA1 (Interchange Acknowledgment)
- 999 (Implementation Acknowledgment)
- 277CA (Claim Acknowledgment), which provides claim-level acceptance or rejection details.
Collectively, the acknowledgements inform the submitter regarding structural validity, syntax conformance to the X12 implementation guide, and individual claim results. The claim can be accepted into adjudication or rejected, depending on the claim details.
Conversely, for billing teams, EDI reporting in healthcare identifies claim-related errors before they turn into denials. Unfortunately, missing out on EDI acknowledgements is one of the most common, yet preventable, reasons for revenue disruptions.
EDI Transactions in Healthcare
According to the CMS Adopted Standards and Operating Rules, ASC X12 Version 5010 is the standard format for electronic healthcare transactions. However, retail pharmacy transactions are an exception, since they employ the National Council for Prescription Drug Programs (NCPDP) Telecommunications Standard Version D.0.
Core HIPAA-Mandated EDI Transaction Types
The core HIPAA-mandated transaction types for EDI in medical billing are as follows:
| X12 Set | Purpose | Direction |
|---|---|---|
| NCPDP D.0 | Retail pharmacy claim and related transactions. | Pharmacy to health plan. |
| 270 / 271 | Eligibility, coverage, or benefit inquiry and response. | Provider to payer & payer to provider. |
| 276 / 277 | Claim status request and response. | Provider to payer & payer to provider. |
| 278 | Healthcare services review (prior authorization) | Provider to payer. |
| 834 | Benefit enrollment and maintenance | Sponsor to health plan |
| 835 | Healthcare claim payment / electronic remittance advice. | Payer to provider |
| 837P / 837I / 837D | Healthcare claim, which applies to professional, institutional, and dental claims. | Provider to payer. |
Quick Insight: Originally, the HIPAA-approved EDI standards were published in 2000.
Electronic Data Interchange Workflow in Healthcare
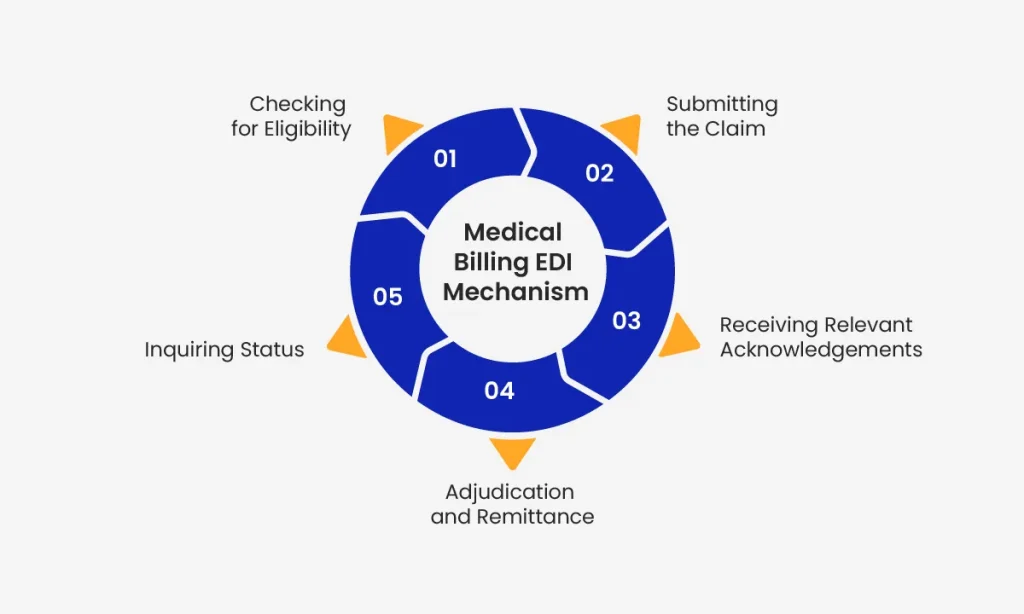
The following is a breakdown of what the typical EDI workflow looks like in healthcare:
1. Checking for Eligibility (270/271)
Initially, during the EDI process, practices submit an inquiry to the payer to confirm the coverage. The confirmation may be required on or before the service date.
2. Submitting the Claim (837)
Once the service has been provided, the practice management or electronic health record (EHR) system prepares a HIPAA-compliant 837 file.
This file is then shared with a clearinghouse, which reviews the information. In other cases, the file may be submitted directly to the payer for reimbursement.
3. Receiving Relevant Acknowledgements (TA1, 999, 277CA)
Next, the receiving system (payer or clearinghouse) returns a series of acknowledgments for:
- Structural validity
- Per-claim acceptance
- Syntactic compliance
4. Adjudication and Remittance (835)
Once the claim has been adjudicated, the payer provides a comprehensive electronic remittance advice (ERA). The ERA can be automatically posted to accounts receivable systems, streamlining payment reconciliation.
5. Inquiring Status (276/277)
There are certain cases where claims may stall. Here, the practice can inquire about the claim status electronically instead of reaching out to the payer.
State-Specific EDI Requirements Providers Should Know
Typically, people still get confused about the ASC X12 Version 5010 because it is the federal standard. Many assume all state Medicaid programs implement it uniformly, but that is not the case.
Instead, each payer or state Medicaid program publishes its own EDI companion guide. These guides provide implementation details in addition to the X12 implementation. The following are some notable state-specific EDI requirements to consider in healthcare:
Texas Medicaid (TMHP)
According to the guidelines from Texas Medicaid Healthcare Partnership 837I Acute Care Companion Guide, Texas Medicaid allows one ISA/IEA envelope and one GS/GE per ISA. This applies to one per file and has a cap of 5,000 transactions per batch. Additionally, direct submitters must complete testing in the TMHP Test Environment, and TMHP provides Edifecs-based self-testing/certification support.
New York Medicaid (eMedNY)
According to the New York State Medicaid Companion Guide, the eMedNY Provider Test Environment only allows ASC X12 Version 5010. It has a limit on real-time test traffic, i.e., 50 claims per file.
NYS DOH has also adopted the 837 Professional standard for Non-Emergency Transportation billing, while the 837 Institutional standard is applicable to Managed Care Capitation Premium billing. It is important to note that these functions are not HIPAA-regulated, yet have been adopted.
California Medi-Cal Dental
According to the Medi-Cal Dental EDI Companion Guide, direct-submitting providers can only submit up to five EDI files per day. Additionally, for certifications, there must be 15-20 HIPAA-compliant test transactions.
These transactions should cover specific scenarios, such as:
- Share-of-cost
- Multiple dates of service
- Incoming 837 claims with more than 50 service lines are rejected
- Health coverage
- Attachments
Quick Insight: All of these Medi-Cal requirements follow federal X12 standards. Therefore, an 837 claim that may be valid otherwise can be rejected if it doesn’t follow the state’s companion guide. Hence, it is a must to review state-specific details before making a decision.
EDI Integration Benefits in Healthcare
The following are some of the benefits of EDI integration in healthcare:
Standardized Payments
According to an HHS guide, approximately 400 proprietary formats for claims were being used before HIPAA introduced its standards. With the help of EDI, the payment methods were standardized, consolidating them into a single national standard.
Lower Administration Expenses
Complicated payment methods posed a serious administrative burden earlier. Fortunately, CMS’s administrative simplification focused primarily on switching to electronic transactions to reduce the involved costs.
Quicker Reimbursements
Manual claim filing involved time-intensive and tedious workflows, like faxing. Fortunately, with electronic claim submissions and 835 remittance posting, this timeline is much shorter. The reimbursements are now processed in a matter of days in many cases.
Electronic methods also make the cash-to-payment cycle safer and more effective compared with paper.
Compliance Enforcement
Providers experiencing compliance issues with a trading partner can file a complaint through the CMS Administrative Simplification Enforcement and Testing Tool (ASETT).
Important Note: Providers must always maintain a documented and compliant chain of custody for all claims. This can be documented via TA1, 999, and 277CA acknowledgments, to ensure 100% electronic data exchange.
EDI Implementation Challenges & Solutions
Implementing EDI in medical billing has its challenges, but professionals can resolve them with the right solutions. Here’s a quick overview of these challenges and how to tackle them.
Standard Changes in the Future
According to the HHS Final Rule published March 24, 2026, ASC X12 Version 6020 standards apply to claims attachments transactions (X12N 275 and 277). These standards take effect on May 23, 2026, with a compliance deadline of May 26, 2028. So, billing professionals should prepare.
Solution
The best way moving forward is to budget for multi-year vendor and workflow upgrades now. This can greatly reduce costs and ensure streamlined operations in the future.
Connectivity and Security
EDI exchanges typically handle sensitive health information and connectivity protocols. These internal systems must always comply with the HIPAA Security Rule. However, achieving this goal might not be as easy for every practice.
Solution
Encrypted exchange and a signed Business Associate Agreement are two of the fastest methods to overcome this challenge. Moreover, we also recommend practicing least-privilege access for trading partner credentials.
Companion Guide Drift
Companion guides may vary for each payer, and following specific guidance is a must. Practitioners and billers must understand situational rules and take necessary steps to mitigate this issue.
Solution
The best way to counter this challenge is to maintain a payer-rule library and treat companion guide updates as release events.
Acknowledgment Fatigue
EDI in healthcare requires several acknowledgements that professionals must read in a timely manner. However, many times, 999 and 277CA files may go unread, which negatively impacts claims. Therefore, professionals should employ the following solution:
Solution
Opt for automated ingestion and route every rejection to an accountable owner with a same-day service level agreement (SLA).
Turn EDI Compliance into a Revenue Advantage
EDI is no longer an option in healthcare; it is a regulatory foundation that your revenue cycle relies on. If a practice treats EDI as a “set-it-and-forget-it” process and fails to review 999 acknowledgments, it risks revenue loss due to missed errors, companion guide mismatches, and delayed claim corrections.
If your in-house team is unable to handle EDI compliance, switching to NeuraBill’s medical billing and coding services can help you secure accuracy with every transaction.