Have you ever visited a physician, and the first thing they do is inquire about your health? They usually do this while checking your records. Healthcare providers rely on medical records for clinical and operational purposes, but what is the ideal duration for medical record retention?
According to the HIPAA Journal, in 2024, 14 data breaches affected more than 1 million healthcare records. This was a serious concern, and even though medical record-keeping has evolved, certain gaps persist.
Therefore, we will cover every crucial detail about medical records retention, including HIPAA requirements, state-specific retention laws, control and disposal of medical records, and common record-keeping errors that healthcare providers make. So, let’s begin with the HIPAA requirements.
HIPAA Medical Record Retention Requirements
The Department of Health and Human Services states that HIPAA does not have a declared retention period for medical records. However, certain compliance-related documents, policies, and procedures should be retained for a period of 6 years.
The reason? Record retention is state-specific and may vary from region to region.
Therefore, retention requirements in Georgia may differ from those in Texas, and so on. Does this mean medical professionals should not consider HIPAA medical records retention requirements?
Quite the opposite, actually, professionals must learn the medical records retention requirements and state-specific laws before maintaining and destroying documentation.
Digging Deeper into HIPAA Requirements
According to the HIPAA Journal:
| Specific documents must be maintained and preserved for at least six years. This duration is from the date of creation or their last period of effect (whichever occurs later or more recently). |
However, clarifying which documents fall under this category is necessary to prevent unwanted violation of HIPAA state-specific requirements.
According to the HIPAA Privacy Rule, individuals can access their files or amend their Protected Health Information (PHI) legally, as long as the information exists in a designated record set.
However, covered providers and entities must provide the patient with an accounting of disclosures of PHI for the last six years (from the time of request). Moreover, the disclosure should include specific details such as:
- Recipient
- Description
- Purpose
- Date
Similarly, professionals must also retain the privacy practice notices, policies, complaints, and other details related to the Privacy Rule for the same period.
Medical Records Retention Laws by State
The American Medical Association (AMA) recommends using medical considerations to determine the optimal time to keep medical records.
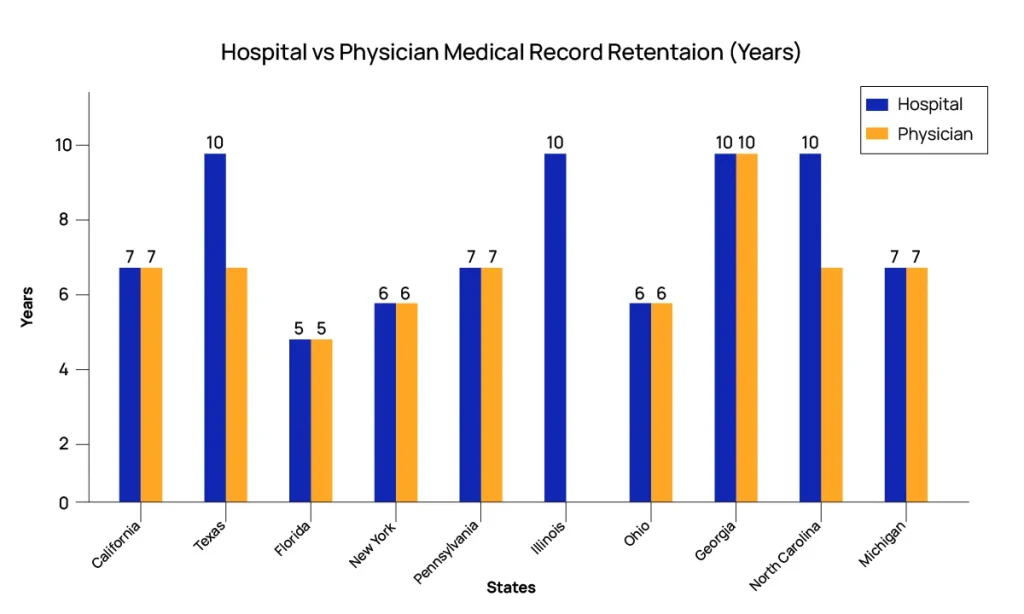
However, this can be confusing. Therefore, here is a comprehensive breakdown of the medical records retention laws of states with the highest population. Please refer to your specific state to avoid violations and penalties.
| States by Population | Hospital Retention | Physician Retention | Minor Records | Governing Authority |
|---|---|---|---|---|
| California | 7 years following discharge | 7 years from last encounter | Age 19 or 7 years | 22 CCR § 72543 |
| Texas | 10 years from the last treatment | 7 years from the last treatment | Age 21 or 7 years | 22 TAC § 163.2 |
| Florida | 5 years from last contact | 5 years from last contact | Standard period applies | Fla. Admin. Code 64B8-10.002 |
| New York | 6 years following discharge | 6 years since last visit | Age 21 or 6 years | 10 NYCRR § 405.10 |
| Pennsylvania | 7 years following discharge | 7 years following discharge | Age 28 | 28 Pa. Code § 115.23 |
| Illinois | 10 years since creation | No single statute; varies by provider type | Age 23 or 10 years | 210 ILCS 85/6.17 |
| Ohio | 6 years post-discharge | 6 years post-discharge | Age 20 or 6 years | Ohio Admin. Code 3701-83-11 |
| Georgia | 10 years since creation | 10 years following discharge | Age 23 | Ga. Comp. R. & Regs. 511-7-1-.10 |
| North Carolina | 10 years since the last service | 7 years since the last service | Age 30 | N.C.A.C. 13 B. 3903 |
| Michigan | 7 years | 7 years from service | Age 25 or 15 years | MCL 333.16213 |
Important Notes
- Iowa adheres solely to Medicaid-specific guidelines.
- Michigan law (MCL 333.16213) mandates a 15-year retention applicable to specific sensitive records.
- Check the retention requirements for your specific state, as they are subject to change.
Disclaimer: State laws vary by provider type, record type, and payer requirements. Always verify with current state statutes and legal counsel.
Control & Disposal of Medical Records
Now that we understand medical records retention laws by state, it is necessary to learn about the control and disposal of medical records.
Can medical professionals dispose of documents immediately? If yes, what is the recommended way to do it? Let’s get to the answers.
Medical Record Control and Disposal
According to the American Academy of Pediatrics, records may be destroyed only after the applicable retention period has passed, provided no litigation, audit, or investigation is pending.
If any state or other applicable law is absent, the PHI must be destroyed in a way that leaves no possibility for the information to be reconstructed.
In other words, once the documents are destroyed, individuals or entities should not allow any unauthorized use or disclosure of PHI, intentionally or unintentionally.
Disposal of Electronic PHI
The HIPAA Security Rule outlines requirements for media reuse and disposal. According to this rule, any electronic or digital hardware or media containing PHI must be properly sanitized before reuse.
Similarly, workforce members responsible for supervising or participating in PHI disposal should have appropriate training for disposal (according to the prescribed procedure and policies).
Note: We recommend reviewing Guidelines for Media Sanitisation tounderstand its application.
State-Specific Regulations
In addition to HIPAA, some states may have their own medical records retention policy that must be followed. Certain states (e.g., Kentucky, Arizona) require patient notification prior to record destruction, depending on provider type and circumstances.
Special Considerations
In rare cases, patient information relevant or required during an open investigation or audit should be preserved for a longer period. The same applies to the retention of medical records for litigation concerning the patient. Some examples may include:
- Medicare audits
- RAC audits
- OIG investigations
Similarly, records must not be destroyed if litigation is anticipated or ongoing (litigation hold).
Therefore, it is imperative to research the latest laws and state-specific regulations before healthcare providers destroy PHI or other medical records.
Documentation of Medical Records Destruction
The entity or individual responsible for destroying a patient’s medical records must report the following information:
- The signatures of the supervisors and witnesses of the destruction.
- Date and destruction method.
- Inclusive dates.
- Description of the disposed records.
- A statement of record destruction.
Medical Record-Keeping Errors by Healthcare Providers
Record-keeping errors have serious implications for patient health, treatment, and journey. According to the American Society of Clinical Oncology Journal, poor record-keeping practices lead to approximately 28% of medical errors.
Therefore, medical practitioners must steer clear of medical record-keeping errors, including:
Inaccurate or Incomplete Documents
Healthcare providers can sometimes add inaccurate or incomplete details to the patient’s documents. This leads to misdiagnosis, extensive treatment periods, resource wastage, and higher treatment costs.
Moreover, incorrect documentation can also result in legal action against a medical facility or service provider.
Outdated Information
Healthcare providers may not always update relevant patient information. For instance, it should be recorded when a patient’s treatment plan was adjusted after an assessment of their latest medical condition.
Poor Integration Systems
Sometimes, healthcare providers may employ a weak record-keeping system or network. This network gap increases the likelihood of inaccuracies in patient data.
Inaccurate Reporting
Medical facilities or health practitioners may also commit record-keeping errors resulting from the billing team’s mistake. For instance, if medical billers report an inaccurate modifier, CPT code, or other procedure detail, the patient record will be compromised.
Improve Medical Record Accuracy & Compliance with NeuraBill
Misunderstanding of medical records retention policies poses serious challenges, as retention periods vary by state, provider type, and patient category, but in many cases, this duration is at least six years, though it varies by state and patient category.
Providers can then destroy the records, but as per the guidelines discussed in this article. Violating these policies can lead to serious ramifications, which is why caution is necessary. Healthcare practices may consider acquiring medical billing and coding services from professionals, like NeuraBill, to ensure compliant and secure record retention.