The U.S. healthcare system greatly relies on physicians, and according to the Federation of State Medical Boards (FSMB) Physician Census, there were 1,082,187 licensed physicians in the U.S. in 2024. Physicians applying for hospital privileges, payer enrollment, or employment within a health system must undergo credentialing and submit supporting documents. These documents may include their:
- State license
- Residency certificate
- Medical school diploma
- Board certification
However, the reliability of the submitted documents can always be a matter of dispute. For starters, the photocopies may be altered, or the provided credentials may be fake. Therefore, primary source verification (PSV) serves as a foundational requirement within physician credentialing standards established by accrediting organizations.
PSV is more than an option or a formality. Instead, it is a required process with a proper structure, controlled by enforceable standards.
Importance of Primary Source Verification for Physicians
But first, what is primary source verification?
The National Committee for Quality Assurance (NCQA) defines PSV as:
Credential verification of the practitioner via primary source, recognized source, or a contracted agent.
Utilization Review Accreditation Commission (URAC), another leading accreditation body, mandates the PSV as a foundational component of the Credentials Verification Organization (CVO) Accreditation standard.
So, what does all of this mean? PSV refers to the actual source, which can be the:
- Certifying body
- Medical school
- State licensing board
The primary requirement is to confirm that a provider’s credentials are up-to-date, genuine, and unencumbered. But what role does it play in billing? Let’s find out.
Why Primary Source Verification in Credentialing for Physicians Matters
Credentialing a sanctioned provider or not knowing that a credentialed provider is a part of a federal exclusion list or has their license revoked can lead to significant risks.
Regulatory Requirement
The CMS Conditions of Participation (CoPs), codified at 42 CFR 482.12, require hospitals to ensure all personnel meet state and local requirements and hold a license prior to providing patient care.
These requirements generally involve verifying licensure and qualifications directly from primary or approved verification sources before patient care privileges are granted.
List of Excluded Individuals
The OIG’s List of Excluded Individuals/Entities (LEIE) lists providers who are no longer members of federal healthcare programs, such as Medicaid and Medicare. Therefore, billing services rendered by an excluded provider may expose organizations to Civil Monetary Penalties (CMPs) and overpayment liability.
These penalties apply even if you bill unknowingly and may result in significant CMP liability for each item or service billed. Moreover, according to the OIG’s Special Advisory Bulletin, OIG requires screening LEIE once a month, and states that the screening:
“Best minimizes potential overpayment and CMP liability.”
Remember, after 2011, the CMS regulations stated in 42 CFR 455.436 require monthly LEIE checks.
National Practitioner Data Bank
Hospitals are generally required to scan the National Practitioner Data Bank (NPDB) during the initial privileging process and at least every two years thereafter.
Moreover, this check is required every two years (even if the practitioner is on the staff). The NPDB serves as a federal repository containing reports related to:
- Adverse licensure actions
- Malpractice payments
- Clinical privilege restrictions
Patient Safety Mechanism
More than compliance, primary source verification in credentialing is a mechanism for patient safety. How? Well, reviewing and confirming a physician’s qualifications is a direct and effective tool to ensure that a licensed and competent practitioner provides patient care.
Primary Source Verification of Credentials – Requirement
According to the published standards as well as the NCQA’s Comprehensive Guide to Credentialing Programs (2025), here is a list of what is needed during primary source verification.
License to Practice
Confirming license details is the most fundamental requirement for primary source verification. Every provider must have a current and valid license in the state where they are practicing for the credentialing decision.
According to the NCQA, the state medical board (depending on the provider’s practice region) must help with directly verifying the license.
DEA or CDS Certification
Prescribing controlled substances is a vital responsibility among practitioners. Thus, it requires organizations to review existing and active Drug Enforcement Administration (DEA) certificates and any applicable state Controlled Dangerous Substances (CDS) registration.
In addition to the state registry, the DEA database needs to be consulted for certifications.
Important Note: Some states, such as Maryland, New Jersey, New York, Texas, and Massachusetts, require a separate CDS registration, in addition to the federal DEA registration.
Board Certification Status (BCS)
The BCS should be verified directly with the applicable certifying body. However, verification may be performed through recognized certifying bodies, including the American Osteopathic Association (AOA) and the American Board of Medical Specialties (ABMS).
Work History
Credentialing organizations and payers commonly require providers to submit at least five years of employment and affiliation history. This information should also include gaps in practice.
According to NCQA standards, work history may be reviewed through a documented curriculum vitae review, although organizations may also contact prior employers or affiliated institutions directly.
Training and Education
The provider’s education and training are necessary for credentialing and practicing, and according to NCQA’s FAQ, if a healthcare provider has a board certification verification, the residency or medical school should not be verified separately.
The certifying board verifies the education before it awards the certification. However, expired board certifications may also help with the education verification requirement.
Why? This is because the education data remains the same, even if the board certification is no longer valid.
Medicare and Medicaid Sanctions and Exclusions
Organizations can verify Medicare and Medicaid sanctions from SAM.gov, along with OIG LEIE. However, it is necessary to screen against both exclusion databases.
State Licensing Sanctions and Disciplinary Actions
Sanctions can only be reviewed with the help of primary sources. These may include relevant state medical boards and the OIG. Organizations can use these sources to check for:
- Disciplinary actions
- State-level restrictions on licensure
- Limitations on the scope of practice
Malpractice History
Another requirement of primary source verification is inquiring about the physician’s malpractice history. Providers are generally required to disclose malpractice history covering the previous five years. Credentialing organizations must gather this information themselves if unavailable and should include the duration of residency and fellowship.
Moreover, the NCQA permits organizations to receive this information from the NPDB.
The following table covers a summary of all the requirements for a quick reminder:
| Credential | Primary or Approved Source |
|---|---|
| State Sanctions / Disciplinary Actions | State medical boards; OIG LEIE. |
| State License to Practice | State medical board (provider’s licensed state). |
| Medicare / Medicaid Sanctions | OIG LEIE; SAM.gov. |
| Malpractice History | National Practitioner Data Bank (NPDB). |
| Education and Training | Medical school, fellowship, or residency (or board cert as proxy). |
| DEA / CDS Certificate | DEA database; state agency registry (if state CDS required). |
| Work History | CV review; direct contact with prior employers and affiliations. |
| Board Certification | ABMS, AOA, or other applicable recognized certifying body. |
Source: NCQA
Primary Source Verification & Credentialing Process
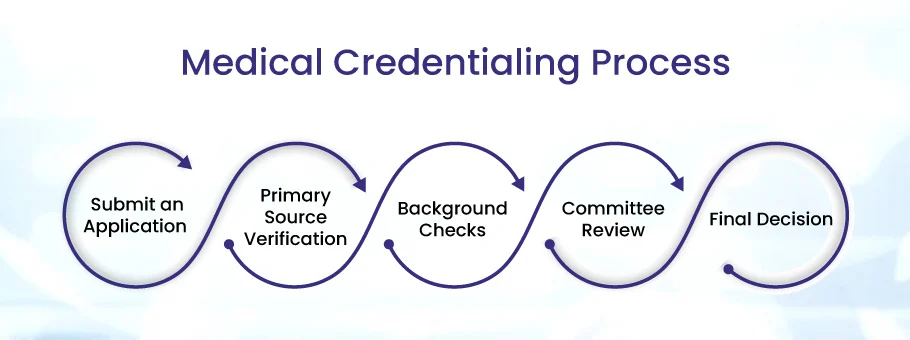
Primary source verification, or PSV for short, is not the only requirement of the credentialing process. It is one phase within the broader credentialing process. However, learning how PSV fits within the credentialing process is a must for handling hospital privileging or network enrollment.
Step 1: Provider Application
The credentialing process begins with the provider submitting an application to the health plan (insurance payer), credentialing organization, or hospital. This application includes the provider’s self-reported:
- Work history
- Training
- Malpractice history
- Licensure
- Education
- Disclosures regarding past sanctions
- Details of previous disciplinary actions
- DEA registration
- Credentials
- Board certifications
Typically, the provider submits this application through the CAQH Provider Data Portal, used by over 1,000 health plans.
Note: The portal is accepted in all 50 states.
Step 2: Primary Source Verification
After receiving the application, the organization starts the PSV for every credentialing element. During the primary source verification for physicians, the organization may directly contact or take information from sources, such as:
- State board
- OIG LEIE
- NPDB
- Medical school
- DEA
- ABMS
All of these sources confirm whether the provider-supplied information matches the issuing authority’s record.
According to the latest 2025 Credentialing Product Suite Standards (effective July 1, 2025), NCQA credentialing verification timelines have been shortened under the updated standards. According to the latest requirements:
- NCQA-Accredited Organizations – Completed within 120 days
- NCQA-Certified Credential Verification Organizations (CVOs) – Completed within 90 days
The updated timelines reflect broader adoption of electronic verification workflows and integrated credentialing systems.
The original 180-day window was set when organizations relied on manual, paper-based verification processes.
Step 3: Credentialing Committee Review
The credentialing committee or review panel is responsible for determining whether the credentials verified during primary source verification meet the privileging criteria or the organization’s in-network enrollment requirements. Per NCQA, CVOs can perform the verification. However, they cannot issue the final determinations for credentialing.
Instead, the credentialing committee is responsible, and the URAC’s Health Plan Accreditation standards shed further light on the matter.
According to this, organizations require a documented credentialing program policy as well as a credentialing committee to review credentials. The committee may also provide credentialing recommendations based on established organizational criteria.
Additionally, according to The Joint Commission, organizations must also keep a documented record of:
- The person conducting verification
- Elements specifically verified
- Verification results
Important: This documentation should be maintained for accreditation survey review.
Step 4: Credentialing Decision
Once the committee review is complete, the provider receives the credentialing decision. According to the NCQA Credentialing Accreditation standards, organizations must hold a fixed recredentialing cycle that the provider can look forward to. Additionally, health plans are required to recredential providers every three years.
Common Challenges in Primary Source Verification
The following is a breakdown of the most common challenges in primary source verification:
State-Level Verification Process Inconsistencies
One of the biggest factors that makes PSV challenging is the national licensure database centralization gaps. The medical board verification systems vary from state to state. Response times and required documentation also vary.
Therefore, if a provider is licensed in multiple states, they need to get a dedicated verification from each board, resulting in additional administrative burden and slower credentialing workflows.
NCQA Verification Timelines
Did you know that, according to the latest NCQA standards, the primary source verification timelines have been reduced to 120 days for accreditation and 90 days for CVO certification? (as stated above).
However, it also means that credentialing committees have a higher workload and need:
- Faster workflows
- Stronger tracking systems
- Improved process efficiency
Volume and Manual Workloads
A large volume of requests is submitted for PSVs, resulting in extensive manual workload and process bottlenecks. Additionally, multi-source verifications also contribute to the problem.
The information must be verified from multiple sources and in some cases across multiple states, which include:
- National Practitioner Data Bank
- Licensing boards
- Federal exclusion databases
- DEA records
- Employment and malpractice history
Continuous Monitoring Requirements
Organizations must continuously and regularly monitor:
- Exclusion lists
- License status changes
- Sanctions
However, manual monitoring processes may become difficult to sustain for large provider networks. Therefore, several organizations opt for automated monitoring systems to avoid compliance oversight.
Documentation Gaps and Data Issues
Organizations may often face multiple inconsistencies during primary source verification when credentialing. These inconsistencies are typically found in provider applications, such as the following:
- Incorrect training dates
- Employment gaps
- Expired certifications
Additionally, bodies such as The Joint Commission also require record verification, making accurate documentation necessary for audit and compliance.
CVO and Delegation Selections
Many times, insurance payers outsource their PSV to CVOs. However, not every organization will handle the credentialing elements precisely.
Therefore, payers must verify the CVO’s NCQA certification status and delegated credentialing scope. Understanding the scope can help avoid and counter compliance gaps and accreditation risks.
Quick Insight: Did you know that only a few organizations hold NCQA CVO Certification for all 11 essential elements?
Streamline Primary Source Verification with NeuraBill
Primary source verification is a demanding and regulated part of physician credentialing. Managing shortened NCQA timelines, multi-state licensure complexities, and documentation standards can be fairly challenging.
It requires up-to-date knowledge of the ever-changing standards, education, and training. Fortunately, acquiring NeuraBill’s medical credentialing services ensures your practice has on-time primary source verification and CAQH profile management.
They can also help you with payer-specific enrollment and re-credentialing cycle tracking, improving your practice’s credentialing efficiency, documentation management, and accreditation readiness.